Self-Reported and Performance-Based Evaluations of Functional Status in Older Women With Breast Cancer
Objectives: To evaluate self-reported and performance-based functional status (FS) in older women with breast cancer according to stage and time of visit during treatment.
Sample & Setting: 72 women with breast cancer aged 78 years or older and receiving any type of treatment at a midwestern outpatient clinic.
Methods & Variables: FS was evaluated using grip strength, the Index of Activities of Daily Living (ADLs), the instrumental ADLs (IADLs) scale, and the Timed Up and Go Test (TUGT). Mixed models were fit for grip strength and the TUGT, and generalized estimating equations were used to fit binary logistic regressions for the Index of ADLs and the IADLs scale. Continuous FS outcomes were evaluated using means and standard deviations.
Results: Cancer stage and time of visit did not affect self-reported or performance-based FS scores. Most participants were considered independent on the Index of ADLs, the IADLs scale, and the TUGT, which did not change significantly between visits. Self-reported measures revealed less impairment.
Implications for Nursing: Monitoring FS using self-reported and performance-based measures can ensure that older patients receive timely support.
Jump to a section
About 7% of people aged 65 years or older and 21% of people aged 85 years or older require some type of help with activities associated with personal care (Centers for Disease Control and Prevention [CDC], 2017). Nearly 9.5 million people aged 65 years or older report difficulty in at least one domain of functioning (CDC, 2021a). In the United States, more than 10% of adults aged 75 years or older require help with activities of daily living (ADLs), and nearly 19% require help with instrumental ADLs (IADLs) (CDC, 2016). People aged 65 years or older who live in poverty are more likely to require assistance with ADLs and are disproportionately affected by comorbidities, such as osteoarthritis, leading to problems with mobility (Stevens et al., 2016; Thompson et al., 2019). Functional status, as opposed to chronological age, is a prime factor in cancer treatment decisions (Soto-Perez-de-Celis et al., 2018).
People aged 80 years or older who are not functionally impaired tend to experience less postoperative complications (Saraiva et al., 2017). Functional impairment is related to mortality at one year following breast cancer surgery (Tang et al., 2018) and is a predictor of severe toxicity (Vázquez et al., 2017). Survival, treatment toxicity, cancer treatment feasibility, treatment decisions, and fewer postoperative complications, as well as older age and type of cancer treatment, are all associated with functional status (Couderc et al., 2019; van Abbema et al., 2017). Anticipating decline can inspire early intervention (Travers et al., 2019) before a person must leave their home or is not offered aggressive treatment for cancer (Bano et al., 2016; Jacobs et al., 2016).
The purpose of this study was to examine self-reported and performance-based evaluations of functional status according to stage of breast cancer over time in women with breast cancer aged 70 years or older. The objectives were to determine whether time of visit (at initial visit, six months, and one year) or cancer stage affect performance-based (grip strength, gait, and balance) and self-reported (ADLs and IADLs) functional status. This research is important because patients with cancer often experience a decline in functional status following cancer treatment (Cabilan & Hines, 2017), and timing of assessment and type of measure are undefined, particularly in advanced stage cancer (Galvin et al., 2019). Understanding the best manner to assess functional status is essential to the care of older people with cancer. Performance-based assessments may be more useful as compared to self-reported functional status in older breast cancer survivors (Winters-Stone et al., 2019); however, other studies have found that a combination of self-reported and performance-based evaluations can better predict important clinical outcomes (Buendia et al., 2020). The current study provides clinical data to help best assess functional status according to stage and time of visit in older women with breast cancer.
Background
Functional Status Assessment
Functional status can be determined by evaluating ADLs (Katz et al., 1963, 1970), which are basic tasks (e.g., bathing, dressing, eating, transferring, using the toilet, continence), and IADLs (Lawton & Brody, 1969), which are more refined tasks (e.g., shopping, housework, transportation, managing finances, cooking). Evaluating functional status helps providers to determine cancer treatment options and general care management strategies, such as the need for physical therapy and stamina for surgery, and to identify those who are at greater risk of surgical complications (Huisman et al., 2017). In the early 1960s, patients in long-term care facilities were evaluated to determine the basic domains of function, which were eventually characterized as ADLs (Katz et al., 1963). Also in the 1960s, executive functioning tasks (IADLs) were identified to help providers to determine the extent of independence of community-dwelling older adults (Lawton & Brody, 1969). The Index of ADLs and the IADLs scale are self-reported measures of functional status that are used as clinical measures and in many research projects. Performance status evaluation is an empirical measure of function, which includes grip strength (Rijk et al., 2016), gait speed, and balance (Podsiadlo & Richardson, 1991), offering a metric on which to base cancer treatment decisions and predict survival (Huisman et al., 2014). Both types of measures are commonly used in caring for older adults.
Functional status limitations are inspired by many variables. Using a combination of self-reported and performance-based evaluations of functional status may help to illuminate ability and detect other problems, such as low muscle mass (Wang et al., 2020). Function can be represented differently depending on self-reported or performance-based measures and age, obesity, presence of pain, and type of joint problems (Wilfong et al., 2020). People may overestimate their ability to bathe or dress independently, and a measure of grip strength or a gait evaluation may help to construct a more objectively defined strategy for management. Understanding how to assess functional status in older patients with breast cancer is important in providing excellent care.
Performance Status Evaluation
A decease of 5 kg in grip strength indicates high risk for all-cause mortality (Celis-Morales et al., 2018). Stronger grip strength is a protective quality for cognitive decline, mobility, and general functional status (Rijk et al., 2016). Weak grip strength is related to impaired quality of life in cancer survivors (Paek & Choi, 2019) and cognitive decline (Yang, Koyanagi, et al., 2018). Grip strength is also related to increased healthcare costs because muscle weakness can be associated with more provider visits, inpatient care, and caregiving needs (Pinedo-Villanueva et al., 2019). Grip strength decreases as age increases, and weak grip strength is associated with lower body weight and poor perception of health, as well as other physical limitations (Forrest et al., 2018). Older breast cancer survivors have lower grip strength scores as compared to people without cancer (Winters-Stone et al., 2019). Grip strength is a predictor of functional decline (Owusu et al., 2017), malnutrition, and survival in older people with cancer (Contreras-Bolívar et al., 2019).
Performance-based functional status evaluations include the assessment of gait and balance, as measured by the Timed Up and Go Test (TUGT) (Podsiadlo & Richardson, 1991), and are considered a vital sign of ability to predict frailty and mortality (Liu et al., 2019). In patients with breast cancer receiving chemotherapy, gait speed and balance are often negatively affected (Monfort et al., 2017). The TUGT can predict survival and treatment-related complications in older patients with cancer (Verweij et al., 2016), which can be improved by exercise in breast cancer survivors (Foley & Hasson, 2016). The TUGT tends to be an easy and quick measure that helps to provide important empirical data that can influence cancer treatment decision-making (Nightingale et al., 2019).
Functional Status in Cancer Care
Functional status evaluations are common in general geriatric care, particularly in the 1980s and 1990s with the use of the comprehensive geriatric assessment (CGA) (Pfeiffer, 1991; Rubenstein et al., 1984). The synergism of general geriatrics and geriatric oncology is reasonable because cancer is a disease of aging (Howlader et al., 2018). In a classic paper, Balducci et al. (1994) defined geriatric oncology as embracing geriatric treatment principles by using the CGA with functioning as a domain, which can detect problems before they become life-limiting. It is well accepted among oncology providers that data on functional status optimize cancer treatment decisions (Soto-Perez-de-Celis et al., 2018), determine symptom burden (Portz et al., 2017), and predict outcomes following surgery (Saraiva et al., 2017) and overall survival (Kenis et al., 2017).
Functional status often declines during chemotherapy; however, nearly half of people report recovery at 12-months post-treatment (Hurria et al., 2019). In patients who were postesophagectomy, functional status returned to baseline in three months, even with high incidence of complications (van Egmond et al., 2020). One-year mortality in people who do not regain functional status capability following cancer surgery is higher as compared to people who regain presurgical function (Schmidt et al., 2018). Improving or maintaining functional status during and after cancer treatment is critical and associated with physical fitness prior to diagnosis (Lee & Park, 2006), better mental health, and the social determinant of income (Van Cleave et al., 2011). For patients receiving care in the hospital, establishing goals during recovery at home can help in regaining premorbid function (Liebzeit et al., 2018).
More data are needed to understand when to assess functional status and what type of measure is most beneficial for use in older people with breast cancer. Self-reported and performance-based evaluations of functional status are clinically useful. Functional status can provide insight into cancer treatment decision-making and predict toxicity, complications, and survival. Optimizing recovery following the diagnosis and treatment of cancer can promote independence in community-dwelling older adults.
Methods
This retrospective observational study evaluated functional status using the Index of ADLs, the IADLs scale, grip strength, and the TUGT at three time points six months apart. To account for the correlation of repeated measures within participants, mixed models were fit for grip strength and the TUGT, and generalized estimating equations were used to fit binary logistic regressions for the Index of ADLs and the IADLs scale.
Sample
Women aged 70 years or older with any stage of breast cancer and receiving any type of treatment were invited to participate in the study. Participants had to be able to read and understand the consent form and speak English. The inclusion criteria consisted of all women who were receiving care in the clinic who consented to participate.
Setting
The study took place at the Stefanie Spielman Comprehensive Breast Center at the Ohio State University in Columbus, which is an outpatient clinical and research facility. Patients from the Cancer Aging and Resiliency (CARE) clinic were invited to participate. The CARE clinic is an outpatient breast cancer clinic focused on people aged 70 years or older who have a diagnosis of breast cancer. The CARE clinic offers an interprofessional team approach (geriatric oncologist, social worker, pharmacist, physical therapist, dietitian, and nurses) to cancer care by offering a CGA every six months to people receiving ongoing care or a second opinion for those who wish to remain with their oncologists. The goal of the CARE clinic is to optimize oncology care by integrating CGAs and an interprofessional team to detect limitations that can negatively affect cancer treatment.
Procedures
The variables of gait, balance, upper extremity strength, ADLs, and IADLs were selected for the study because decreased gait speed and weakening grip strength are associated with a higher likelihood of mortality (Liu et al., 2019), and a third of older patients with cancer report an ADL and/or IADL limitation (Neo et al., 2017). The variables used in this study are commonly used in clinical research to evaluate functional status (Jacobs et al., 2016; Leong et al., 2015; Nightingale et al., 2019).
The data used in this study are part of an ongoing geriatric oncology CGA protocol. All study measures are part of the CGA, and no additional instruments were administered. All CGA data are recorded in the medical record. Patients who presented to the CARE clinic from 2013 through 2018 were invited to participate in the study. The geriatric nurse practitioner (GNP) obtained written consent from the patient. Cancer diagnosis, staging, and treatment information were obtained from the medical record. The GNP completed the study instruments with each patient when they were in the examination room for their oncology examination, which required about 20 minutes.
Data were collected during the first encounter (visit 1), at six months (visit 2), and one year from the initial encounter (visit 3). Grip strength was measured using the Jamar® hydraulic hand dynamometer, with three consecutive grasps per hand. The TUGT was performed in a premeasured area in the clinic. All data were collected by the same GNP. Data were entered into and analyzed using SAS®, version 9.4.
Ethical Conduct
This study was approved by the Ohio State University Institutional Review Board (IRB). The study was explained, and informed consent and Health Insurance Portability and Accountability Act (HIPAA) forms were signed by all participants according to the standards of the IRB. Participants were not compensated for inclusion in the study. Participants were not screened for cognitive deficits prior to informed consent; all participants were able to verbalize understanding of the purpose of the study and read the informed consent and HIPAA forms. Based on their reading and verbalized understanding of the consent form, all participants were determined to have had decision-making ability and were competent to consent on their own behalf (Office for Human Research Protections, 2016).
Instruments
The TUGT evaluates the ability to rise from a seated position, ambulate 9.8 feet, and return to the seated position (Podsiadlo & Richardson, 1991). The TUGT is correlated with falls (Shumway-Cook et al., 2000), with a cut point for fall risk at 12 seconds or more (Bischoff et al., 2003). Interrater reliability is high at r = 0.98. The TUGT has also correlated with the Berg Balance Scale (r = –0.55) (Berg et al., 1992), gait speed (r = –0.55), and Barthel Index for ADLs scores (r = –0.51) (Collin et al., 1988). The TUGT was conducted as a one-time test of a person rising from an armchair and walking 9.8 feet, with the use of an ambulatory device for those who needed assistance.
The Index of ADLs includes six items (bathing, dressing, transferring, feeding, continence, and toileting). If a person is dependent in any of the tasks, assistance and rehabilitation are generally explored (Katz et al., 1963). A limitation in any one of the activities indicates a functional deficit.
The IADLs scale evaluates more refined activities (Lawton & Brody, 1969), such as using the telephone, getting to places beyond walking distance, grocery shopping, doing laundry, cleaning, performing housekeeping activities, self-administering medications, and managing money. The IADLs scale has eight items, and the patient earns 1 point for being able to perform a task without assistance and 0 points for requiring some assistance or being completely unable. Dependence is defined by any one task that requires assistance (Lawton & Brody, 1969), which indicates a functional deficit.
Grip strength was measured in the right and left hand using the Jamar hydraulic hand dynamometer (Patterson Medical, 2013). While sitting and holding the dynamometer with the arm extended at 90 degrees, patients are asked to squeeze as hard as possible, giving three consecutive grips several seconds apart in the right hand first and then in the left hand. The three grip strength measures on each hand were averaged, yielding a single score. The grip strength measurements predict limitations in mobility for the patient (Massy-Westropp et al., 2011; Wang et al., 2018). The average score of the three grip strength measures for each hand can be compared to normative data in the Jamar owner’s manual (Patterson Medical, 2013). The cut point of 37 kg or less was used to determine strength difficulties for the left and right hands of women (Patterson Medical, 2013). Norms for grip strength in the dominant and nondominant hands for women aged 70–74 years are 27.5 kg in the 90th percentile (Wang et al., 2018).
Analysis
To address the specific aims of the study, the demographic characteristics of the sample were summarized using descriptive statistics. For the continuous outcomes (left hand grip strength, right hand grip strength, and the TUGT), repeated-measures binary regression models were used for each outcome. Visits, defined by the encounter number in the CARE clinic (initial encounter, six months, and one year), and stage of cancer were model predictors, with visit fit as a class variable. Means and standard deviations were evaluated for the continuous functional status outcomes by cancer stage and visit. The aims were to test the statistical significance of the effect of the visit and stage of disease on each outcome and, if statistically significant, estimate the change in outcome between visits.
For the ordinal outcomes (ADLs and IADLs), there were relatively few participants who scored other than independent on measures of functional status. Therefore, each variable was arranged into a dichotomy, with the top ADLs and IADLs scores (6 and 8, respectively) set to 0 and all other scores set to 1. Using these transformed outcomes, logistic regression models of the probability of having the status of “not independent” were fit. For the Index of ADLs and the IADLs scale, generalized estimating equations were used to fit repeated-measures binary logistic regressions.
Results
The mean age of participants (N = 72) was 77.9 years. Many of the women did not have metastatic disease (n = 56), 52 women were diagnosed with infiltrating ductal carcinoma, and 42 underwent a lumpectomy. Twenty-seven participants were diagnosed with stage I breast cancer, 19 were diagnosed with stage IV, and 18 were diagnosed with stage II (see Table 1). 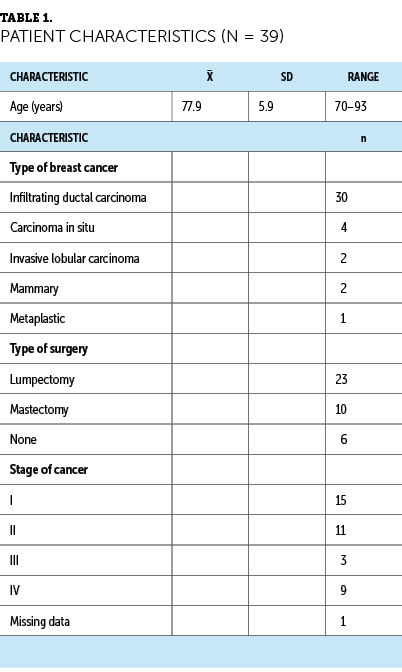
Table 2 presents the means and standard deviations of the continuous functional status outcomes by cancer stage and visit. There was no clear pattern in the relative size of the means for left and right hand grip strength over time. Mean scores on the TUGT were nearly the same at visit 1, and mean scores for advanced disease were smaller thereafter. 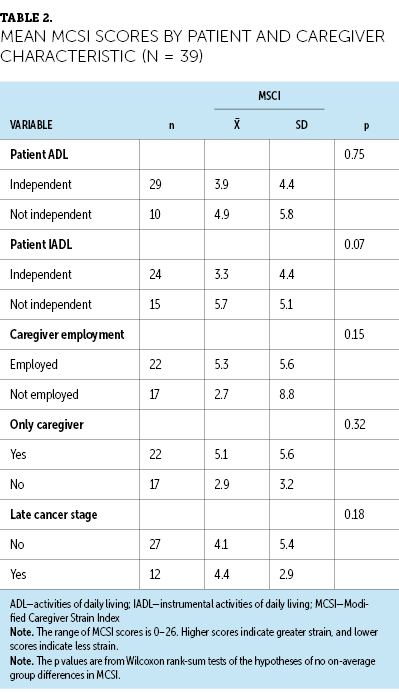
Table 3 presents the frequency of ADLs and IADLs indicators by cancer stage and visit. Frequencies for those categorized as “not independent” were calculated. There were relatively more participants with advanced disease categorized as “not independent” over time on the Index of ADLs. For the IADLs scale, there were relatively more participants with advanced disease categorized as “not independent” at all time points. However, the small sample sizes at visits 2 and 3 for those who were “not independent” should be noted. 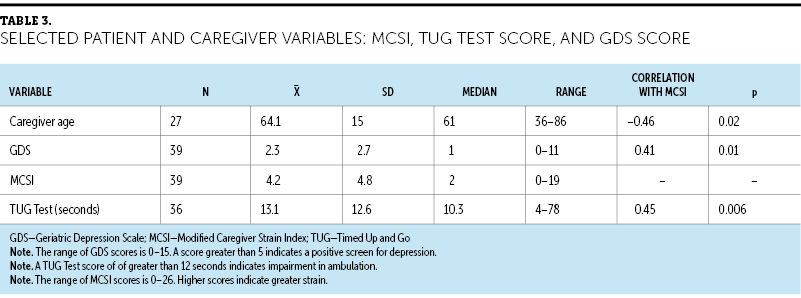
Mean scores on the Index of ADLs and the IADLs scale were 5.5 and 7.1, respectively, which does indicate that many participants required some supervision with activities. Thirteen participants had one or more ADL limitation, and 21 had one or more IADL limitation. The mean TUGT time was 11.5 seconds; however, 17 participants did have a time of 12 seconds or longer, which indicates impairment. Forty-four participants had a right-handed grip strength of 37 kg or less (norm for people aged 70–75 years), with a mean of 34.8 kg in the right hand, and 43 had a left-handed grip strength of 33.8 kg, indicating weakness (see Table 4). 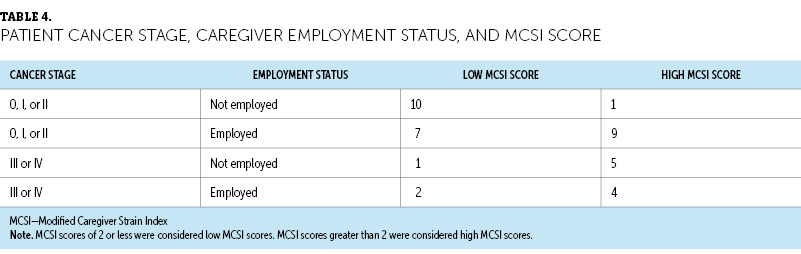
Models of functional status were fit to test whether disease status had predictive value. In the models, cancer stage was coded as 1 if the stage was III or IV and as 0 if the stage was 0, I, or II. Two models were fit. Model 1 included visit, cancer stage, and the interaction of visit as predictors. Model 2 included visit and cancer stage as predictors. For the continuous outcomes (left hand grip strength, right hand grip strength, and the TUGT), repeated-measures binary regression models were fit with a random effect for each variable. All p values associated with cancer stage were not statistically significant. The lack of statistical significance of the model 1 interaction term indicated that there was no evidence that time moderates the effect of stage (i.e., there is no evidence that the effect of stage on functional status depends on the time of the visit). The lack of statistical significance of the main effect of stage in model 2 indicated that there was no evidence that stage affects functional status as measured by grip strength or the TUGT. For the Index of ADLs and the IADLs scale, as with the continuous outcomes, no p value associated with cancer stage was statistically significant. There was no evidence that cancer stage affects ADLs or IADLs. Table 5 presents the p values for model 1 and model 2 predictors. 
Discussion
Many participants were independent on the Index of ADLs, the IADLs scale, and the TUGT, despite a mean age of 77.9 years and 19 participants having stage IV breast cancer. The results indicated that breast cancer stage does not affect functional status, as measured by grip strength, the TUGT, the Index of ADLs, and the IADLs scale. Mean grip strength in the right and left hand was reflective of impairment among participants. Most older people are not functionally impaired and live independently in the community despite the presence of comorbidity or illness (Administration on Aging, 2020). Despite functional status limitations, many older adults can live in the community, particularly if they are married and/or have support in the home (Matos et al., 2018).
Except for grip strength, most scores were not reflective of functional impairment, suggesting that some participants have a functional reserve. Functional reserve contends that an individual has the stamina to resist or recover from an insult, such as a diagnosis of breast cancer and cancer treatment (Colloca et al., 2015). When functional reserve is critically reduced, frailty pursues, and resilience is eroded (Balducci, 2013). Functional reserve can be enhanced by physical activity, which can slow sarcopenia and delay the development of disability (Marzetti et al., 2017). The extent of functional reserve can affect the ability to live independently following a cancer diagnosis and treatment.
Based on the results of this study, there was no evidence that the timing of assessments or cancer stage affected functional status scores on self-reported or performance-based evaluation measures. Functional status tends to improve following oncology surgery in cases where the recovery is not complicated (Van Cleave et al., 2011). Following breast cancer surgery, physical activity level is often reduced depending on the extent of surgery (Harrison et al., 2021). In a study by Couwenberg et al. (2018), 25% of participants who underwent more extensive surgeries, such as abdominal surgery for colorectal cancer, experienced postoperative complications, and older people were more likely to experience some type of functional impairment six to twelve months following diagnosis.
Grip strength in the left hand decreased over time among participants with stage 0, I, or II breast cancer, particularly between visits 1 and 3, but not significantly. For participants with stage III or IV breast cancer, grip strength in the left and right hands fluctuated over time. Other studies also found a small reduction in grip strength among patients with breast cancer who were receiving aromatase inhibitors (Van der Weijden-Van Doornik et al., 2017). Grip strength is affected by the side of surgery, particularly on the nondominant side (Perez et al., 2018). Other considerations for a weaker grip strength can be osteoarthritis (Wen et al., 2017), chemotherapy administration (Marques et al., 2020), and mastectomy (Zabit & Iyigun, 2019).
Scores on the TUGT remained about the same for participants with stage 0, I, or II breast cancer, but the scores were better at visit 2 and 3 as compared to visit 1 for those who were diagnosed with stage III or IV breast cancer. Gait speed is reduced for many people with breast cancer, and balance is impaired as compared to normative values (Hsieh et al., 2019). The TUGT is clinically helpful in caring for older people with breast cancer and is used to predict fall risk (Blackwood & Rybicki, 2021).
Based on the means of the functional status measures, ADLs and IADLs did not reveal the extent of disability indicated by grip strength. This is consistent with the literature, in which many people tend to overestimate functional ability, particularly after a surgical procedure (Dayton et al., 2016). Exclusively relying on self-reported measures may not provide a full depiction of functional status (Stevens-Lapsley et al., 2011). Using a combination of self-reported and performance-based evaluation measures may help to understand functional ability and aid in appropriate management strategies.
The small sample size, particularly during visits 2 and 3, is a limitation in this study. In addition, tracking surgery, reconstruction, treatment type, and toxicities could have been important to the results. Another limitation was that grip strength was identified by the right and left hands and not by the dominant and nondominant hands.
Implications for Nursing
Functional assessment should be part of oncology care for older patients. Following surgery, some patients can experience functional decline, and preoperative functional assessments can help to identify people at higher risk of dependence (Ghignone et al., 2020). Identifying people who are less likely to functionally recover can help providers and patients make treatment decisions (Huisman et al., 2017). People who are physically active prior to breast surgery have a better chance of functional recovery (Yang, Sokolof, & Gulati, 2018). Following hospitalization, premorbid function affects outcomes over time (Sáenz et al., 2020). Encouraging physical activity in older patients with cancer is an important element of the cancer management plan.
A tailored exercise plan can not only preserve function, but also help with addressing effects of chemotherapy (Duregon et al., 2019). Healthy aging through the promotion of an active lifestyle, social inclusion, and well-being contributes to better hematologic profiles and enhanced quality of life (Caseiro et al., 2020). A diagnosis of breast cancer should inspire nurses to recommend an active lifestyle and wellness behaviors, such as diet and nutrition, in survivorship plans. The National Cancer Institute (2020) recommends 150–300 minutes of aerobic activity weekly, as well as balance and muscle training exercises. Prescribing an individualized exercise program using Active People, Healthy Nation recommendations can be influential (CDC, 2021b). Writing a prescription for exercise using the Frequency, Intensity, Time, and Type guidelines can enhance adherence and potentially improve outcomes (CDC, 2021b; Garvey et al., 2020).
Evaluating functional status using grip strength, the TUGT, Index of ADLs, or the IADLs scale can be conducted by a nurse or advanced practice nurse in inpatient or outpatient settings. The Hartford Institute for Geriatric Nursing (www.hign.org) offers resources on all types of assessments and has several options for functional status measures. The site also provides information on how to conduct various assessment tools, interpretation, and clinical use. Nurses can conduct the assessment, document the results in the medical record, and report to the healthcare team. 
Conclusion
There is no evidence that cancer stage or timing of evaluation on self-reported or performance-based measures affects functional status in older women with breast cancer. Most participants were considered independent on the Index of ADLs, the IADLs scale, and the TUGT, which did not change significantly between visits. Grip strength in both hands did change between visits but not significantly. Self-reported functional measures revealed less impairment as compared to the performance evaluation measure of grip strength. Monitoring functional status regularly and using a combination of self-reported and performance-based measures during cancer care can be helpful in providing timely support that can maintain independent living for older people.
About the Author(s)
Janine Overcash, PhD, CNP-APRN, FAANP, FAAN, is a professor of clinical nursing in the College of Nursing at the Ohio State University in Columbus; Hannah Riffle, BSN, RN, is a labor and delivery nurse at Saint Joseph Hospital in Denver, CO; and Loraine Sinnott, PhD, is a research professor in the College of Nursing, and Nicole Williams, MD, is an assistant professor in the Stephanie Spielman Comprehensive Breast Center, both at the Ohio State University. No financial relationships to disclose. Overcash and Williams contributed to the conceptualization and design and completed the data collection. Overcash and Sinnott provided statistical support and analysis. Riffle and Williams contributed to the manuscript preparation. Overcash can be reached at overcash.1@osu.edu, with copy to ONFEditor@ons.org. (Submitted February 2021. Accepted May 26, 2021.)